Invasive muscle bladder adapted treatment with Elekta Unity
Contributors: Genesis Care St Vincent’s Clinic Sydney; Jeremy de Leon, Sandy Sampaio, Monique Heinke, Claire Pagulayan, Jack Aylward, Louise Hogan, David Crawford, Stacy Alvares, Michael Jameson.
Institution: Royal Marsden NHS Foundation Trust
Location: London UK
Authors: Ian Hanson, Gillian Smith, Shaista Hafeez
Overview
Within the first few months of using their Elekta Unity MR-Linac, St Vincents Genesis Care in Sydney, Australia were using the deformable adaptive workflow to treat bladder cases within 30 minutes. Fastest time 25.5 minutes. To decide on this workflow, they utilized the MR-Linac Consortium network and collaborated with the Royal Marsden NHS Foundation Trust, London, UK.1
Introduction
A 72-year-old patient, affected by muscle invasive bladder carcinoma self-referred herself for treatment on Unity.
The bladder is subject to large inter fractional position, shape, and size variation. Significant changes in the shape, size and position of the bladder during radiotherapy (RT) treatment for bladder cancer have been correlated with high local failure rates; typically due to geographical misses. To account for this, historically large population-based planning target volume margins are added around the target volumes in conventional RT to achieve acceptable target coverage; however, this increases the volume of healthy tissue irradiation and does not always successfully mitigate against geographical target misses1.
MRI defined bladder tumor is up to 50% smaller than defined on CT2.
Adapt to Shape (ATS) or deformable plan adaptation and motion management on Unity allow the team to adapt to the varying bladder position, shape and size.
Magnetic resonance radiation therapy (MR/RT) presents an opportunity to graduate to much smaller margins. The current standard is to use a ‘Plan of the day’ approach but the benefit of daily adaptive treatment with MR/RT will ultimately be to address huge margins for such a variable structure fraction to fraction.
Prescription
The clinician prescribed a radical whole bladder dose of Bladder 55Gy ICRU 50/62/83 2.75Gy 20 fractions (1 per day, 10 per fortnight).
Technique
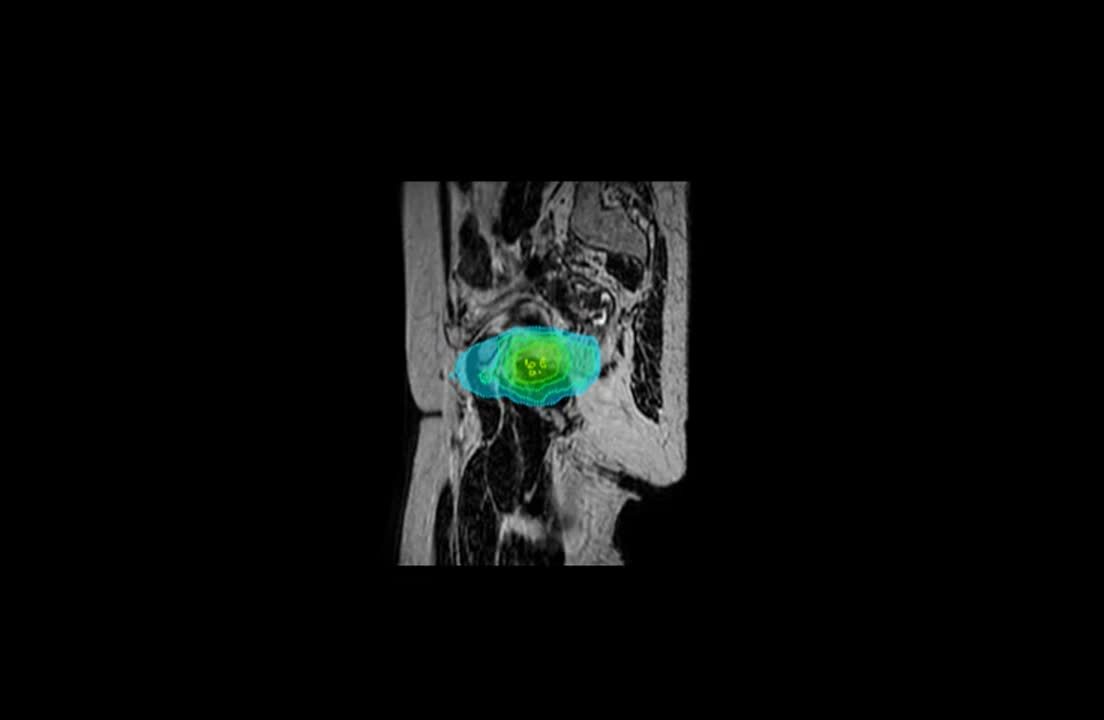
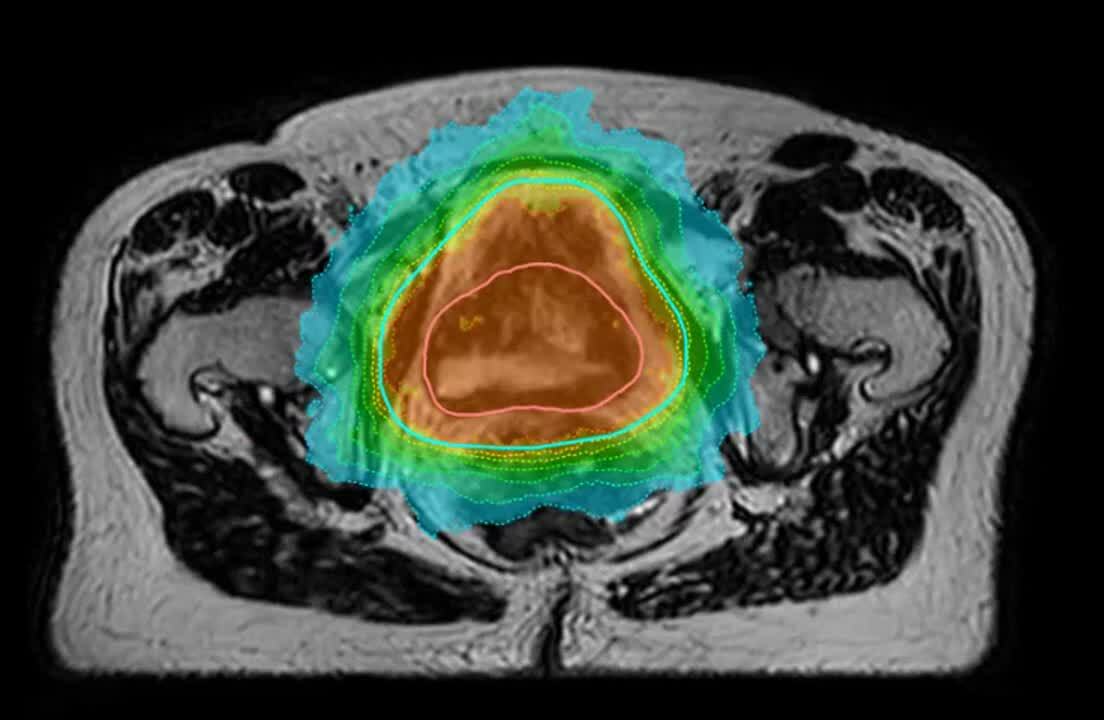
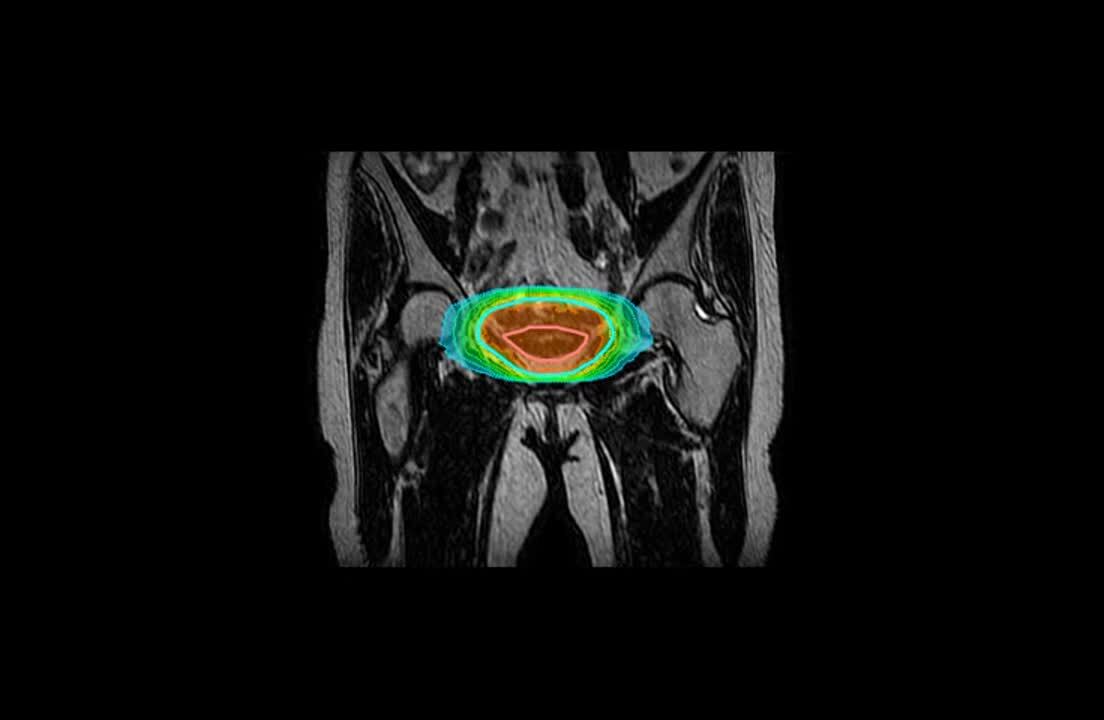
The planning process included MR fusion using MRI scans taken 30 minutes apart to inform the PTV. A daily MRI before treatment (in this case Daily T2 3D Tra 2min MR sequence) provides superior soft tissue contrast without any additional ionising radiation risk. When combined with online adaptive re-planning capabilities, Unity offers the opportunity to adapt the plan at each fraction to the anatomical changes seen to the PTV and to surrounding healthy tissue including the bladder and rectum.
Beams
The mBeam plan consisted of 11 IMRT beams, providing online adaptive robustness for plan adaptation as needed based on the daily anatomy, and online MR Cine motion monitoring of the PTV.
Report
Consistent daily quality results throughout all the fractions were delivered.
References
- Hunt A, et al. Feasibility of magnetic resonance guided radiotherapy for the treatment of bladder cancer. The Royal Marsden NHS Foundation Trust, London, UK. Clinical and Translational Radiation Oncology 25 (2020) 46-51.
- Kibrom AZ, Knight KA. Adaptive radiation therapy for bladder cancer: a review of adaptive techniques used in clinical practice. J Med Radiat Sci. 2015;62(4):277-285. doi:10.1002/jmrs.129 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4968556/