Bilateral thalamotomy with Leksell Gamma Knife for Essential Tremor
Case: Essential tremor in left and right hands
Contributor: Jean Regis, MD, Professor of Neurosurgery at Aix Marseille University and Head of the Stereotactic, Functional Neurosurgery and Radiosurgery Department at La Timone University Hospital, Marseille, France
Overview
Essential tremor (ET) is the most frequent movement disorder. It is a neurological disorder characterized by uncontrollable tremor (shaking) which can occur in different parts of the body, especially in the hands. ET generally presents bilaterally. Treatments for ET include medications, surgical implantation of deep brain stimulation electrodes (DBS) and radiosurgery.
For historical reasons, symmetrical bilateral surgery of the ventral intermediate nucleus (VIM) was not considered during many years due to early experience of side effects including gait, balance, dysarthria, verbal fluency and cognitive impairment problems when radiofrequency thermo coagulations and DBS were performed bilaterally.1-3 However, more recent studies suggest that bilateral radiosurgery is safe in selected patients who present with no complications or impairments in the neurophysiological tests after the first treatment.4-6 A minimum of 2 years gap between the two treatments are mandatory.
This 72-year old right-handed male was diagnosed with ET at a young age, with a past history of ET in the family. At the age of 50, the disability from the tremor got worse, see video in figure 1.
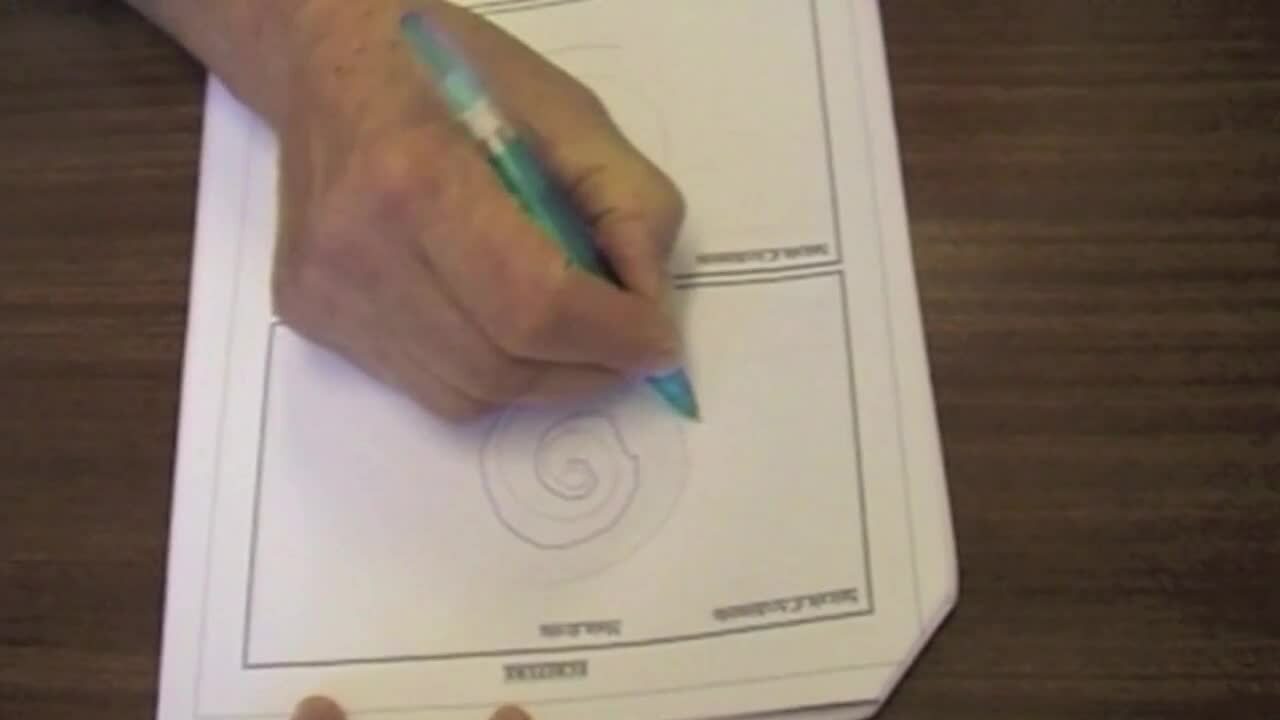
Figure 1 Video showing the tremor affecting both hands.
The patient’s spiral drawing test in figure 2 shows that the tremor was affecting both the left and right hands. In the test, the patient was asked to follow the pre-drawn line. The tremulous lines represent the lines drawn by the patient.

Treatment protocol 1st procedure
First Gamma Knife radiosurgery procedure
On April 15, 2010, the first Gamma Knife radiosurgery procedure was performed. A left VIM target was selected to treat the right-hand tremor, see figure 3.
The stereotactic frame was applied in the morning followed by MRI imaging and treatment planning. The prescription dose was 130 Gy (100% isodose line) delivered in a single shot using a 4 mm collimator. The planning took 10 minutes and the treatment 90 minutes. The patient could return to home the day after.

Follow up after first Gamma Knife radiosurgery treatment
After six months follow up in October 2010 there was no change visible on the MR image and the patient experienced no or very minimal improvement.
At one year follow up in April 2011 the tremor in the right hand had disappeared completely and the patient was extremely satisfied, see video in figure 4.
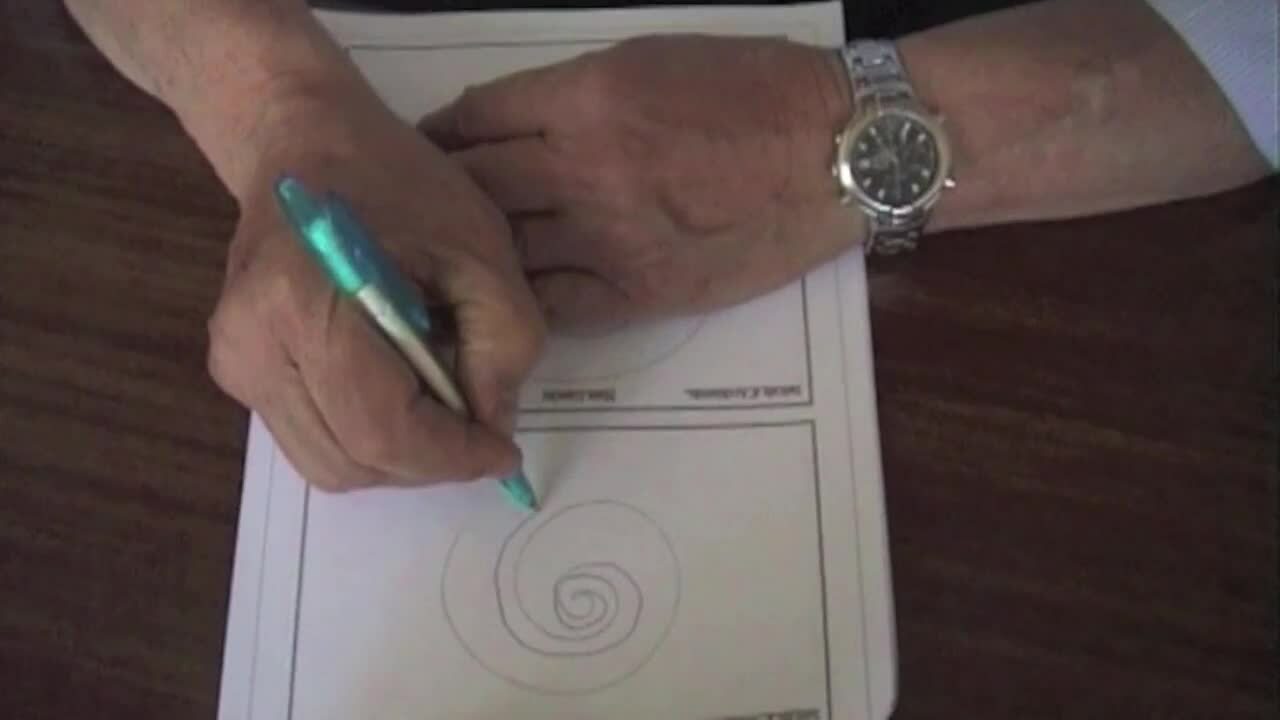
Figure 4 Video showing that the tremor in the right hand has disappeared.
The spiral drawing test in figure 5 shows that the right hand is now working normally.

Treatment protocol 2nd procedure
Second Gamma Knife radiosurgery procedure
After thorough neurophysiological testing of the gait, balance, dysarthria, verbal fluency and cognitive functions after the first treatment, the result showed no complications or impairments in any of these functions. On July 10, 2014, four years after the first treatment, a second Gamma Knife radiosurgery procedure was performed to treat the tremor in the left hand targeting the right VIM, see figure 6.

The prescription dose was the same as in the first treatment, i.e. 130 Gy (100% isodose line) with a single shot using a 4 mm collimator.
The planning took 10 minutes and treatment time was 90 minutes and the patient could also this time return to home the day after the treatment.
Follow up after second Gamma Knife radiosurgery treatment
The patient was followed up 3, 6, 12 and 24 months after the treatment. On July 9, 2015, one year after the second Gamma Knife treatment, the tremor in the left hand had disappeared completely, see video in figure 7.
Figure 7 One year after second Gamma Knife treatment
Results
The outcome after the two treatments was 100% improvement in both hands.
The table in figure 8 compares the tremor assessment before the two treatments and 12 months after treatments. The result in the table demonstrates a dramatic improvement after the radiosurgical treatment. This excellent result is permanent 6 years after the second treatment.
| Before 16/11/2009 | 1 Year 4/05/2011 | At GK2 8/7/2014 | 1y GK2 9/07/2015 | ||
| Functional Disability* | Right | 38/75 | 0/75 | 0/75 | 0/75 |
| Left | 26/75 | 30/75 | 0/75 | ||
| Amplitude of the tremor | Right | 13/24 | 1/24 | 0/24 | 0/24 |
| Left | 18/24 | 11/24 | 16/24 | 5/24 |
Table showing tremor assessment scores before and after treatments
*A lower score means a decreased level of disability

Conclusions
Bilateral Gamma Knife VIM thalamotomy offers a safe and effective alternative for DBS and thermal coagulation like radiofrequency or high focused ultrasound of ET in selected candidates. The advantages with Gamma Knife radiosurgery compared to DBS are that Gamma Knife radiosurgery is a non-invasive treatment with no risk of bleeding or infection that may occur with DBS surgery.
Gamma Knife radiosurgery for ET is a clinically proven treatment method with over 1,600 patients treated worldwide*.
*Leksell Gamma Knife Society
References
- Speelman JD, Schuurman R, de Bie R, Esselink R, Bosch DA. Stereotactic neurosurgery for tremor. Mov Disord. 2002.
- Moriyama E, Beck H, Miyamoto T. Long-term Results of Ventrolateral Thalamotomy for Patients with Parkinson's Disease. Neurol Med Chir (Tokyo) 39, 350-357. 1999
- Alomar, S, King, NKK, Tam, J et al. Speech and language adverse effects after thalamotomy and deep brain stimulation in patients with movement disorders: A meta-analysis. Mov Disorder 2017 Jan;32(1):53-63.
- Young RF, Li F, Vermeulen S, Meier R. Gamma Knife thalamotomy for treatment of essential tremor: long-term results. J Neurosurg. 2010 Jun;112(6):1311-7.
- Ohye C, Higuchi Y, Shibazaki T, Hashimoto T, et al. Gamma knife thalamotomy for Parkinson disease and essential tremor: a prospective multicenter study. Neurosurgery. 2012 Mar;70(3):526-35; discussion 535-6.
- Niranjan A, Raju SS, Monaco EA, Flickinger JC, Lunsford LD. Is staged bilateral thalamic radiosurgery an option for otherwise surgically ineligible patients with medically refractory bilateral tremor? J Neurosurg. 2018 Feb;128(2):617-626.