Organ preservation aims to treat rectal cancer without removing the rectum. Instead of immediate radical surgery, patients receive conservative treatment, such as chemoradiotherapy (CRT). If a clinical complete response is achieved, surgery may be safely omitted, and patients enter a structured surveillance program, often called “watch and wait.” This approach, introduced by colorectal surgeon Habr-Hama, helps avoid surgical morbidity, preserves anorectal function, and maintains quality of life4.
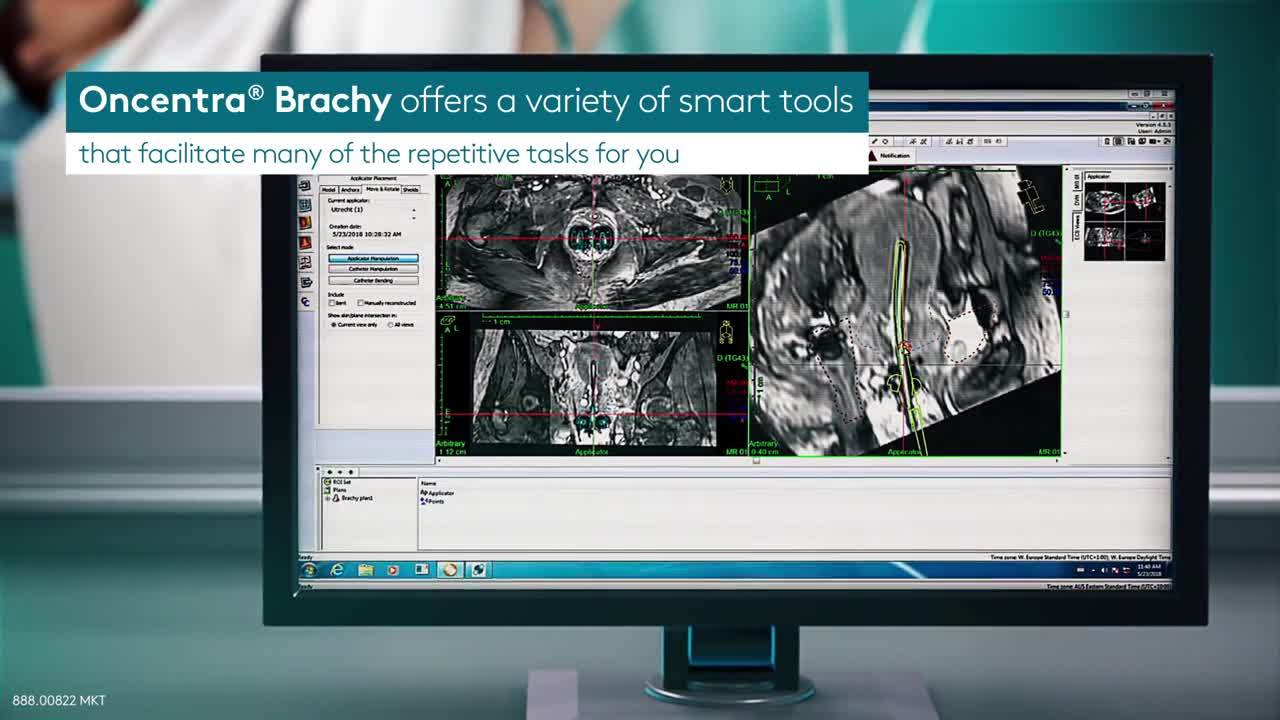
Endorectal high-dose-rate (HDR) brachytherapy is used as a dose-escalation boost in combination with CRT, supporting strategies that aim to enhance tumor response and facilitate organ preservation in selected patients. HDR brachytherapy treatment is guided primarily by tumor imaging, especially MRI, which helps select eligible patients and improves tumor visualization. Treatment planning is performed using 3D CT simulation.
Organ preservation strategies incorporating endorectal HDR brachytherapy are now reflected in clinical guidelines. The European Society for Medical Oncology (ESMO) 2025 guidelines for localized rectal cancer recommend that, for patients with T1–T2 N+ or T3 N0–1 tumors <5 cm in the middle or lower rectum, CRT combined with dose escalation using endorectal brachytherapy may be considered as a treatment option (Level I evidence)5.